
OTBA for Class 11th Biology Theme 2-2015
OTBA Biology for Class 11th Theme 2
OPEN TEXT MATERIAL
Theme 2– Environmental Sanitation
Abstract:
“Environmental sanitation is a biggest public health issue in India. Present interventional studies on
environmental sanitation in the country highlighted the significance of prioritizing control strategies.
Research referred to the appropriate cost – effective intervention strategies and their result oriented
implementation in Indian context is a great challenge. These strategies need to be structured
according to the need of the country. This material gives an insight about the present status of
sanitation, alarming situations, the efforts put in for its betterment and need of the hour.”
“…..No one should spit or clean his nose on the streets. In some cases the sputum is so harmful that
the germs are carried from it and they infect others with tuberculosis. At some places spitting on the
road is a criminal offence. Those, who spit after chewing betel leaves and tobacco, have no
consideration for the feelings of others. Spittle, mucus from the nose, etc., should also be covered
with earth.
“Near the village or dwellings, there should be no ditches in which water can collect. Mosquitoes do
not breed where water does not stagnate. Where there are no mosquitoes, the incidence of malaria is
low. At one time, water used to collect around Delhi. After the hollows were filled, mosquitoes were
greatly reduced and so was malaria.”
Mahatma Gandhi, ‘Navjivan’ Dated 2-11- 1919
Bapu was deeply distressed by stark contradiction existing between our religious precept –
“Cleanliness is next only to godliness” – and the ubiquitous deficit of environmental sanitation and
hygiene in India.
 Environmental sanitation envisages promotion of health of the society through providing clean
Environmental sanitation envisages promotion of health of the society through providing clean
surroundings and thus breaking the cycle of communicable diseases. It depends on diverse factors
that include sanitary habits and status of people, availability of different types of resources,
innovative and suitable technologies according to the requirement of the society, socio-economic
status and development of the country, cultural factors associated with environmental sanitation,
political commitments, capacity building of the sectors concerned, social factors including
behavioural pattern of the community, adopted legislative measures etc. Our Country is still lagging
far behind as compared to many countries in this field. Contaminated sanitary conditions are
terrible in India and need a sensitive sanitary awakening similar to the one which took place in
London in 19th century. Improvement in sanitation requires innovative strategies and target
oriented interventions with follow-up assessment/s. The need of time is to analyze the existing
system of environment sanitation with respect to its structure and functions and to decide the
control strategies according to the requirement. These priorities are principally important because
of issue of water constraints, speedy population expansion, health problems, unequal distribution
of water resources, administrative problems, industrialization and urbanization, migrating
population, and rapid economic escalation.
Water, hygiene, and sanitation are the most important basic requirements which are needed to
ensure public health. Still approximately half of the world’s population i.e. 2.4 billion people, lacks
proper sanitation and one sixth of the world’s population i.e. 1.1 billion people, has no availability of
safe and affordable drinking water. Lack of these basic necessities is intense in poorer, developing
countries, and affects both, urban and rural areas. According to the WHO (World Health
Organization), 80% of diseases, is associated with deficit of access to safe drinking water,
inadequate and inappropriate sanitation, and poor hygiene conditions.

As per estimates, in 2006, inadequate sanitation cost India around $54 billion or 6.4% of the
country’s GDP. Over 70% of this economic brunt or about $38.5 billion was health-related,
diarrhoea followed by acute respiratory infections accounted for 12% of the health-related impacts.
Evidences suggest that all sanitation and water improvements are cost-effective in all developing
sub-regions of the world.
Societal demand for water is increasing rapidly in India, mainly due to urbanization and according
to estimations made by 2025, approximately 50% or more of the country’s population will be residing
in cities and towns. Rising incomes population increase, and industrial growth are responsible for this
theatrical shift. National urban sanitation policy of the year 2008 was the recent development to
quickly promote sanitation in all cities across the country. Ministry of Urban Development, India
commissioned the survey as an element of its National urban sanitation policy in November 2008.
Local government institutions in rural areas, which are in-charge of maintaining and operating the
infrastructure, are seen as fragile and lacking in financial resources to perform their functions. In
addition, no big city in India is known to comprise of a continuous water supply system and according
to an estimate, 72% of citizen of Indian still lack access to better sanitation services.
“Our lavatories bring our civilisation into discredit. We like to take an enjoyable bath, but don’t mind
dirtying the wells, rivers and tanks, by whose side we perform ablutions. These practices should be
considered as a great vice. These are responsible for the disgraceful state of villages and the sacred bank
of sacred rivers and for the diseases that spring due to lack of sanitation.”
‘Our Dirty Ways’ by Mahatma Gandhi in Navajivan, 13 September 1925
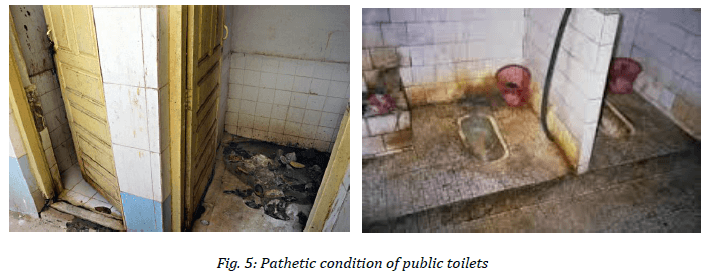
In India, only 36.4% of the entire population have proper toilets, making it one of the weaker
nations for sanitation point of view in the world. This means increased widespread open defecation
which causes contamination of the water resources and spread of diseases transmitted through
insects. In addition, in India, there are dry, or basket-type toilets, which require manual removal of
feces. Currently, India has over 8 million dry toilets, requires 750,000 scavengers every day to
manually remove and cart human excreta for its disposal with no protecting gear. Not only is the
work inhumane, but it is highly dangerous also. The indecent removal of human waste causes
these workers to be infected and thus communicate many diseases to others also. Therefore, such
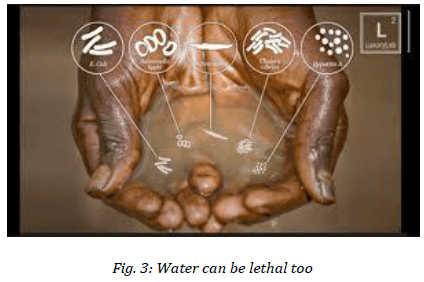
easily preventable diseases as diarrhoea (just a simple action of washing hands with any kind of
soap and water can decrease the number of diarrhoeal disease surprisingly by one-third ),
Cholera, Malaria, Hepatitis and Typhoid are main causes of mortality due to diseases in India and in
other third world countries.
Following are some facts, collected from various sources, prevailing in the country:
India has over 8 million dry toilets, requiring more than one million scavengers everyday to
manually remove and carry human excreta for its disposal.
Over 77% of rural families in the country do not have toilets. (Census 2001)
29% of urban families in India do not have toilets. (Census 2001)
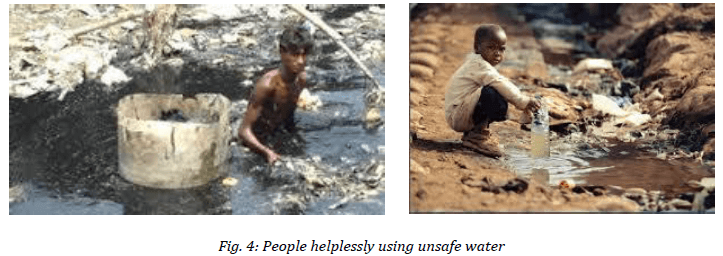
Two out of five people in India do not have access to safe drinking water. (Census 2001)
India spends 73 million working days in a year due to sicknesses caused by lack of sanitation
and unsafe water. (WASH Facts & Figures, 2003)
2.2 million People in developing countries of the world (most of them are children) die every
year from diseases associated with inadequate sanitation and poor hygiene, and lack of access
to safe drinking water. (WASH Facts & Figures, 2003)
In India, only 40% of primary schools have toilets. (DDWS, 2003)
In a survey, it is estimated that approximately half of the world’s hospitals’ beds are occupied
by the patients who are suffering from diseases which are caused either due to poor hygiene or
are water-borne. (WASH Facts & Figures, 2003)
“Any city that would attend to its sanitation in a true spirit, will add to both its health and wealth.”–Mahatma Gandhi
Water and sanitation affect not only to health, but to other vital aspects of life also. The economical
condition of India as a whole is getting affected due to the fact that people are paying for visits to
the doctor and may lose their jobs due to their inability to go to work. In rural areas, the condition
is all the more painful. Education is getting adversely affected when girls drop out from schools
once they attain adolescence because of lack of proper sanitation facility in schools.
Rights of women are also on stake as they are being forced to wait until it gets dark to answer the
nature’s call in order to preserve their privacy. The condition was so poor that the United Nations,
in 2001, declared sanitation as one of its main priorities of the Millennium Development Goals,
aiming to reduce the data by half that lacks sanitation and access to clean water by the year 2015.
In the past, however, it seems that since water and sanitation were majorly a problem of poor, the
crisis has chiefly been ignored and disregarded. It is estimated that diarrhoea, pneumonia, malaria,
and tuberculosis which account for more than 20% of disease burden of the world, receive the
delivery of less than 1% of total private and public funds dedicated to health research.
Not only in case of humans, but environmental sanitation has also a crucial role to play in
maintaining continuity in evolution and advancements in other groups of classification too. All
kinds of flora and fauna on earth, also deserve to inhabit a safe and supportive habitat which is not
being provided to them due to undesired human interventions which result in poor sanitation.
Accumulation of fertilizers in food chains or water cycles can be lethal to them and their future generations. However it is just the ignorance which is accumulating al such problems and it can be easily removed by making the human species aware and by bringing about a behavioural change.
Some government agencies, academic institutions and NGOs are taking innovative steps to either
develop cost-efficient technologies and implementation strategy or to educate and motivate
communities to adopt better/newer ways/technologies for the purpose. The Environmental
Sanitation Institute in India, along with its NGO, has been continuously working for last 40 years to
implement appropriate sanitary and hygiene practices like washing hands, using toilets for
excretion, using soakage pits for waste water, and using trashcans for garbage collection through
both construction and training to improve these conditions.
A number of innovative approaches to improve sanitation and water supply have been tested in the
country in the year 2000. These include community-led total sanitation, public–private
partnerships to improve the continuity of urban water supply in Karnataka, and demand-driven
approaches in rural water supply since 1999.
Complete sanitation drive gives strong stress through capacity building and hygiene education for
effectual behaviour change, Information, Education, and Communication (IEC) with involvement of
community-based organizations and Non-Governmental organizations (NGOs), Panchayati Raj
Institutions (PRIs) etc. The key intrusion areas are individual household toilets, Anganwadi toilets
supported by Rural Sanitary Marts (RSMs), community sanitary complex, school sanitation and
hygiene education (SSHE), and production centres (PCs). The main goal of the government of India
(GOI) was to remove the practice of open defecation by 2010. To boost this endeavour, GOI has
launched Nirmal Gram Puraskar to acknowledge the efforts in terms of cash awards for completely
covered PRIs and those institutions and individuals who have contributed notably in ensuring full
sanitation treatment in their area of operation. The scheme had been implemented in rural areas
considering district as a unit for operation/implementation.
A recent research highlighted that policy shift to take account of better household water quality management to complement the advancing expansion of coverage and up gradation of services would appear to be a cost-effective health intervention in many of the developing countries. Most ofthe interventions (including hygiene and water quality) were found to be decreasing the amount ofillness due to diarrhoea significantly, with the biggest impact being seen for hygiene and householdtreatment interventions. Plans to improve water quality at the household level are more effectivethan those at the source site. It is sad to know that in developing countries, public health concernsare generally raised on the institutional setting, such as environmental sanitation, hospitals,municipal services etc. There is a sort of disinclination in acknowledging the home as a site of equalimportance along with the public institutions, in the chain of communication/transmission ofdiseases in the society/community. Members of management system of community and home hygiene must act in unanimity to optimize return from hard work to support public health.
A survey through profound interviews with more than eight hundred households in the city of Hyderabad in India concludes that, a substantial proportion of poor households would spend in water and drain network connections, even if provided with market (not concessional) rates of financing.
WHO Guidelines related to drinking water quality give emphasis on an integrated approach for
assessment of water quality and its management from source to consumer. These guidelines also
emphasize upon prevention of contamination and quality protection, and advises to be
participatory and proactive, and addresses the needs of those who have no access to piped water
supplies in their community. The guidelines call attention to the maintenance of microbe quality to
prevent waterborne infections as an essential objective. In addition, they address protection from
chemical toxicants including other contaminants of civic health concern.
When conditions of sanitation are poor, water quality improvements may have negligible impact
regardless of amount of contamination in water. If each transmission pathway alone is sufficient to
spread a diarrhoeal disease, single-pathway interventions will have negligible benefit, and
ultimately an intervention will be successful only if all adequate pathways are eliminated. However,
when any pathway is critical in maintaining the concerned disease, public health efforts have to
mandatorily focus on this critical pathway. The affirmative impact of improved water quality is
largest for families which are living under superior sanitary conditions, with the effect statistically
noteworthy when sanitation is considered/measured at the community level but not significant when sanitation is considered / measured at the household level. Improvement in drinking water
quality will not be effective in neighbourhoods with very pitiable environmental sanitation;
however, in areas which are blessed with better sanitatary conditions in the community, reduction
in the turbidity of coliforms of fecal matter by a remarkable degree, would lead to a 40% lessening
in diarrhoea. Providing means of disposal excreta on their own would be expected to trim down
diarrhoea by 42%, while eliminating excreta from surroundings of houses would lead to a 30%
decline in its cases. The findings report that improvements in the areas, sanitation and water
supply, are necessary if it is needed to improve infant health. These also imply that the condition is
not epidemiologic but behavioural, and economic factors should precisely determine the
precedence in interventions. Another research highlighted that water quality interventions for
water treatment were reported to be more effectual than thought previously, and multiple
interventions (consisting of water quality, sanitation, and hygiene measures) were not more
efficient/impactful than interventions with a single focus. Actual findings have shown that just a
small step – hand washing can reduce diarrhoeal episodes by approximately 30%. This noteworthy
reduction is analogous to the effect of providing safe water in low – income areas.
Lack of supply of safe water, improper disposal of human excreta, poor environmental sanitation,
and poor personal hygiene, are major contributors in perpetuating and spreading diarrhoeal
diseases. Because these diseases are caused by 20–25 pathogens, vaccination, though an attractive
disease prevention strategy, is not practical. However, as most of the childhood diarrhoeas are
caused by Vibrio cholerae, Shigellae dysenterae type 1, rotavirus, and enterotoxigenic Escherichia
coli which have a high morbidity and mortality, vaccines against these organisms are necessary for
the control of spread of epidemics. A strong political will along with appropriate budgetary
allocation is indispensable for the control of childhood diarrhoeal diseases in the country.
Mortality and morbidity, because of waterborne diseases, have not declined proportionately with
increase in accessibility to potable water. More crucially, young children bear a big part of the
burden of these diseases which are resulting from the deficit of hygiene. India still loses between
0.4 and 0.5 million children under 5 years due to these diseases. While infant and under 5 mortality
rates have declined over the years for the country as a whole, in many states, these have stagnated
in few recent years. One of the major reasons is failure to make considerable progress in improving
home and personal hygiene, especially in taking care of newborns and young children.
National water policies are shifting to community-based management approach because local
authorities are in regular contact with users. Historically, national policy shifted from attention to
distribution of investments in the concerned sector for restructuring water agencies and for
building up the competence of private or voluntary agencies. The confined context allows for more
efficient and effectual responses to local conditions.
Local groups and institutions are better equipped to solicit participation at local level. Planning of Local water resource is also very important in fortification of the economic and individual power of poor people in areas under development. Experience of Mahesana, Sabarkantha and Banaskantha, in Gujarat state supports this lesson learned. Some of the major hindrances in Gujarat to water resource improvement were identified as inadequate provision of services due to remoteness of the area, amplified demand for public water services and financial limits of central agencies. Infrastructure is also inadequately maintained.
The agriculture sector accounts for approximately 90 and 95% of ground and surface water in
India, while industry and domestic sector account for the remaining resource. At the same time,
several significant measures are being taken to deal with the abovementioned issues. The National
Water Policy, 2002, on the water resources management front, recognizes the requirement for welldeveloped
information systems at the state and national levels, and gives a strong emphasis on nontraditional
methods for utilization for example inter basin transfers, desalination of brackish or sea water, artificial recharge, as well as conventional water conservation/preservation practices such as rainwater harvesting, etc., to increase resources of usable water. It also advocates treatment of catchment area, watershed management through extensive soil conservation, conservation of forests, and increasing forest cover and check dams construction.
The policy also identifies the latent need for reorganizing and reorienting institutional set -ups for the sector and stresses upon the necessity to maintain existing infrastructure.
Because no broad / comprehensive study on equity concerns relating to sanitation, water supply,
and health had been conducted for the country as a whole, common equity issues that plague the
sector in most of the countries under development, hold true for India also. In addition, any
broad/comprehensive study on sanitation and economical value of the water sector in India also
does not exist.
It is important to reiterate the need for Rural Water Supply and Sanitation [RWSS] and Urban
Water Supply and Sanitation [UWSS] agencies to be operational hand-in-hand with their education
and health counterparts to jointly monitor indicators / parameters of health, poverty, education,
UWSS, RWSS, and equity in order to make important progress in the particular sectors. Existing
health promotion and education series should be made well structured and more effective and
geared towards achieving behaviour changes which are highly needed for the betterment of
hygiene conditions.
Percentage of urban population without proper sanitation in India is 63%. The 11th five year plan
envisaged 100% coverage of urban water, urban sewerage and rural sanitation by 2012. Although
investment in water supply and sanitation is likely to see a jump of 221% in the 11th plan over the
10th plan, the targets do not take into account, the quality of water being provided, or the
sustainability of systems being put in place. Increasing emphasis on use of information technology
applications in management and urban governance to ensure quick access to planning, information
and decision support systems are the key concern areas related to environmental sanitation. Solid
waste management is also progressively seen as more important area in UWSS. Legislation on
municipal waste treatment and management has been passed in October 2000. Some strategies on solid waste management include preparing town-wise master plans, giving training to municipal staff, IEC and awareness generation programme,involvement of community-centered and nongovernmental organizations, setting up and operation of compost plants with the help of NGOs and private sector, enhancement of the holding capacities of some state structures such as State Compost Development Corporations with emphasis on commercial operations and private sector participation. Variety in housing type, density and settlement layout, poverty condition, and access to networking services will lead to different solutions for sanitation in different areas of the city or within the same neighbourhood.
Major challenges are as follows:
Prevention of water from getting contaminated in distribution/supply systems
Growing water scarcity and the exploration of potential for water reuse and conservation
Implementing pioneering low-cost sanitation structure
Providing sustainable water supplies and sanitation for urban and semi-urban areas
Dropping disparities within the regions of the country
Sustainability of services related to management of water and sanitation
The public health challenge inherent in meeting the global targets is ensuring that improvements
necessarily result in access to water and sanitation for crucially at-risk populations. Novel
approaches are required to ensure the availability of low-cost, and locally acceptable water and
sanitation practices and integration of these approaches into existing social institutions such as
education institutes, shopping areas, and health sector.
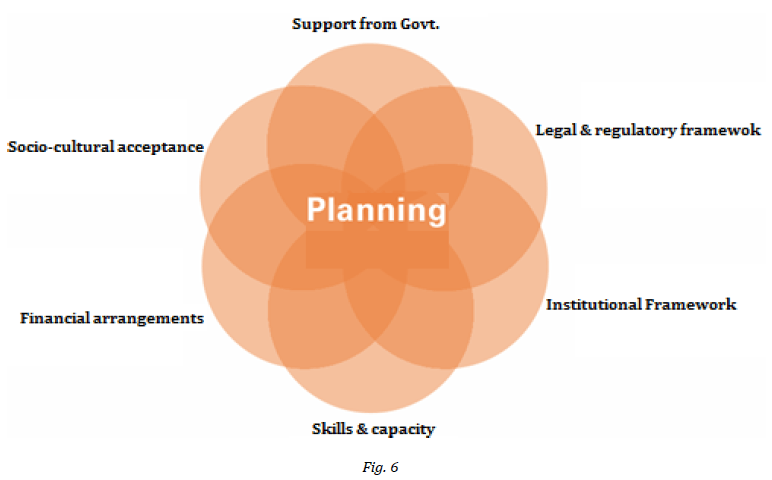
Execution of low-cost sanitation system with lower subsidies, more household involvement, range
of technology options, choices for sanitary complexes for women, drainage systems in rural areas,
IEC and awareness building, involvement of NGOs and local groups, availability of finance support,
human resource expansion, and weightage to school sanitation are some of the important areas
which are to be considered. Also appropriate forms of private sector participation and public private partnerships (PPPs), evolution of a strong sector policy in Indian context, and stress on sustainability with political support and commitment are prerequisites to bring about the change.
The requirements can be communicated schematically as shown below:
But more than anything else, it is required to change the behaviour of people so that they can
sustainably adopt good sanitary practices. However, changing hygiene behaviour is harder than it
may appear at first sight. Since it is related to tradition, environment, culture, and economy, improving existing sanitary practices, involve paying attention to the requirements and desires of the community. In the past, toilets have been built only to be used as storage amenities. In other cases, people have not been educated about how to use and maintain toilets, led to causing them to become unserviceable.

In order to sensitize people towards the needs of the community so that their efforts are successful,
proper training and education is a fundamental necessity. Training that is holistic and practical and
covers all areas should be given each strata from professionals in the field of water and sanitation
to grass root NGO workers, to panchayats of villages to ensure embodiment of concepts as well as
their sustainability.
Many NGOs in the country intend to fulfil this need by providing a centre of excellence for water and sanitation to increase the capacity of field workers in the growth sector and of all related stakeholders. By behaving in this manner, we are sure that we will be able to continue our work in upliftment of the downtrodden, up gradation of rural and urban wellbeing, creation of environmental consciousness, and betterment of the sanitation condition of Environment.
Web links referred:
https://in.news.yahoo.com/dont-urinate-public-gandhi-said-way-back-1925-134804693.html
http://www.vancouverdesi.com/lifestyle/dont-urinate-in-public-gandhi-said-way-back-in-
1925/797567/
http://www.linkedin.com/today/post/article/20140928175615-153568249-gandhiji-s-viewson-
environment-sanitation-hygiene
http://www.gandhi-manibhavan.org/gandhiphilosophy/philosophy_environment_
sanitation.htm
Sample Questions
1. Poor environmental sanitation can lead to adversities in a city. Mention some innovative ways
to spread awareness about them and to improve it to a remarkable level. Maintenance of
environmental sanitation is directly proportional to the health of the society and it is also
responsible for economic escalations. Justify with suitable examples. 5 marks
2. Improved Environmental Sanitation brings about richness and scarcity in biodiversity. Poor
environmental Sanitation brings about richness and scarcity in biodiversity.
Analyze both of the above statements; describe them with suitable examples in support of
each aspect. 5 marks
Marking Scheme
1. Assessed as a whole covering all necessary aspects 5 marks
2. Assessed as a whole covering all necessary aspects 5 marks


















